 AODA Alliance
AODA AllianceACCESSIBILITY FOR ONTARIANS WITH DISABILITIES ACT ALLIANCE
NEWS RELEASE – FOR IMMEDIATE RELEASE
Ford Government Refuses to Make Public Its Bioethics Table Report Recommending Which Seriously-Ill COVID-19 Patients Should Be Refused Critical Medical Care They Need if the Surge in COVID-19 Cases Exceeds Hospital Capacity
October 5, 2020 Toronto: The Doug Ford Government must now end its unjustified secrecy around its plans for Ontario’s most vulnerable patients, if the current surge in COVID-19 cases overloads Ontario hospitals, says a recognized disability advocacy coalition. Deeply disturbing Toronto Star and Radio Canada reports over the last two days, set out below, reveal that the Ford Government refused to make public the report it received last month that recommends how cases should be triaged in such life-and-death situations. The Government-appointed “Bioethics Table” was assigned to recommend how Ontario hospitals should decide which COVID-19 patients should be refused life-saving critical care that they need, and gave the Ford Government their advice in a written report which has been kept secret for three weeks since the Government received it.
“This is part of a much larger pattern of totally inappropriate Ford Government secrecy on this life-and-death issue for Ontario’s most vulnerable. Last spring the Government had issued a secret protocol direction to Ontario hospitals on this subject that was replete with disability discrimination,” said David Lepofsky, chair of the AODA Alliance which has advocated for months on this issue along with other disability leaders and experts. “We’ve told the Ford Government’s Bioethics Table that their earlier proposals for how hospitals should handle this issue are full of human rights violations, but we can’t find out if they acted on our concerns because the Government is keeping their report secret.”
The AODA Alliance has raised with both the Bioethics Table and the Minister of Health the added serious concern that provincial directions to hospitals on this issue should be publicly debated and enacted in a law, and not simply issued in a secret memo to hospitals from some unaccountable level within the Ontario bureaucracy. The Government has not answered these concerns.
It is good that Ontario hospitals have not yet had to engage in triage of critical care patients. However, the troubling spike in COVID-19 infections brings Ontario nearer to a point when that triage must happen, especially if the Ford Government did not use the past six months to ensure that Ontario hospitals have the needed expanded critical care capacity.
“We need Doug Ford to keep his commitments on protecting Ontario’s most vulnerable, and on ensuring complete transparency of his Government’s work on the COVID-19 pandemic,” said Lepofsky. “The Government’s bureaucratic preoccupation with secrecy violates those commitments.”
The Ford Government should now:
- Immediately lift its veil of secrecy and make public the report on critical care triage that it received from its Bioethics Table, and the earlier March 28, 2020 critical care triage protocol that the Government sent to Ontario hospitals and never rescinded.
- Immediately consult the public, including the disability community, on what Ontario’s policy should be in this area.
- Commit that any directions on this issue will be set out in a law, and not simply in a secret memo to Ontario hospitals from some unelected public servant.
Contact: AODA Alliance Chair David Lepofsky, aodafeedback@gmail.com
Twitter: @aodaalliance
For more background on this issue, check out:
- The AODA Alliance’s September 25, 2020 letter to Ontario Health Minister Christine Elliott, as yet unanswered, that calls for the steps listed above.
- The formal written questions to the Ford Government to the same effect, tabled in the Legislature by NDP disabilities critic Joel Harden on September 30,2020 (and which the Government must answer within 24 legislative sitting days after the questions were tabled)
- The August 30, 2020 AODA Alliance final written submission to the Ford Government’s Bioethics Table.
- The April 8, 2020 open letter to the Ford Government on the medical triage protocol spearheaded by the ARCH Disability Law Centre, of which the AODA Alliances one of many co-signatories
- The April 14, 2020 AODA Alliance Discussion Paper on Ensuring that Medical Triage or Rationing of Health Care Services During the COVID-19 Crisis Does Not Discriminate Against Patients with Disabilities
- The May 13, 2020 ARCH Disability Law Centre’s Analysis of the March 28, 2020 Triage Protocol, which the AODA Alliance endorses.
- The July 16, 2020 AODA Alliance Update that lists additional concerns with the revised draft triage protocol. That Update also sets out the Ford Government Bioethics Table’s revised draft triage protocol itself.
- The ARCH Disability Law Centre’s July 20, 2020 brief to the Bioethics Table on the revised draft triage protocol and ARCH’s September 1, 2020 final submission to the Bioethics Table, both of which are endorsed by the AODA Alliance.
- The AODA Alliance website’s health care page, detailing our efforts to tear down barriers in the health care system facing patients with disabilities, and our COVID-19 page, detailing our efforts to address the needs of people with disabilities during the COVID-19 crisis.
Toronto Star Online October 4, 2020
(Note: Also included in the October 5, 2020 print edition of the Toronto Star)
Originally posted at https://www.thestar.com/news/gta/2020/10/04/its-life-and-death-as-ontario-hospitals-face-new-wave-of-covid-19-disability-advocates-want-triage-protocol-released.html
‘It’s life and death’: As Ontario hospitals face new wave of COVID-19, disability advocates want triage protocol released
By Brendan Kennedy Social Justice Reporter
Opposition critics and disability advocates are calling on Ontario’s government to publicly release its COVID-19 triage protocol, which would guide doctors on how to determine who should get life-saving treatment if hospitals are overwhelmed by coronavirus patients.
The purpose of the protocol, which would only be invoked as a last resort if critical care resources needed to be rationed, is to minimize overall mortality by prioritizing patients with the best chance of survival.
The Ministry of Health says the protocol is still being reviewed and will not be made public at this time.
A draft version of the protocol, which was first leaked in March, was criticized for discriminating against people with disabilities. A revised draft was circulated this summer as the province solicited feedback from certain groups, including some disability advocates, who said the revised draft was still discriminatory.
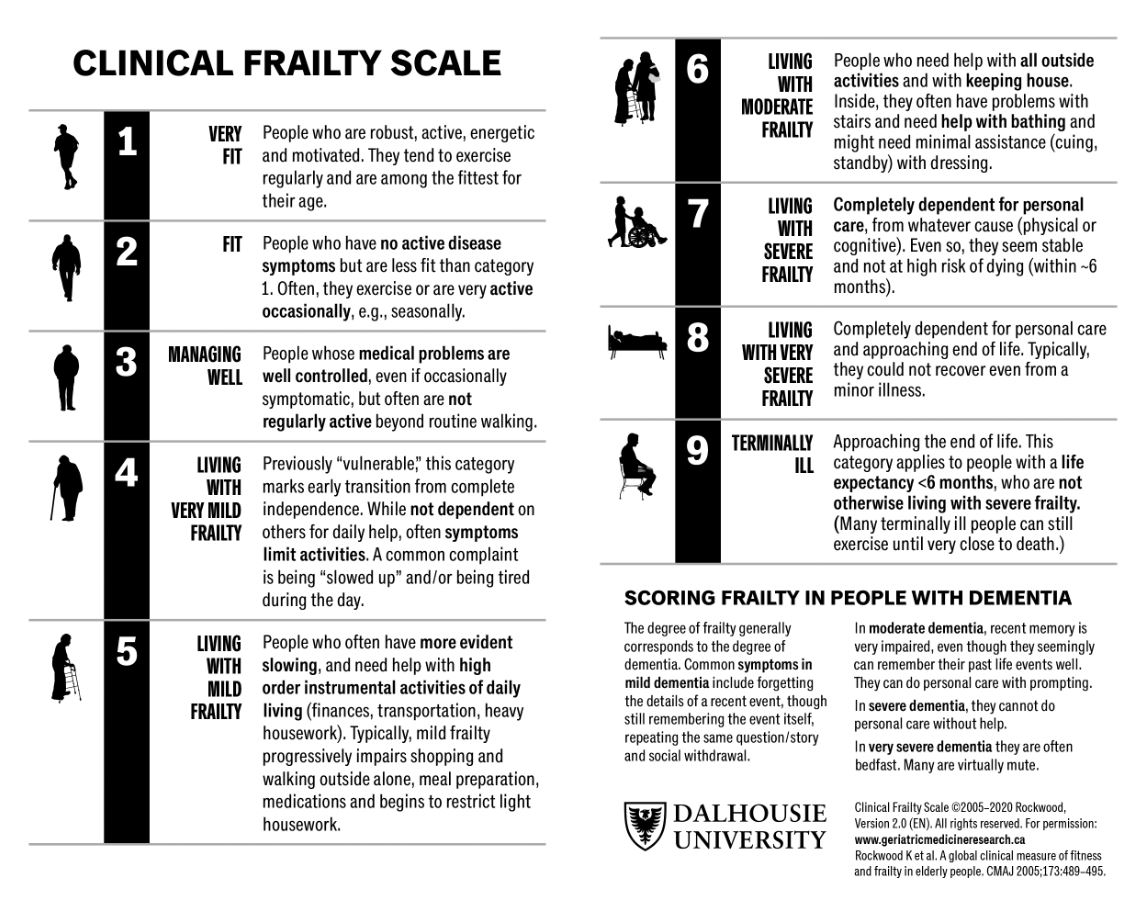
Among their main concerns was the inclusion in the protocol of the Clinical Frailty Scale, a nine-point grading tool originally designed to assess the relative frailty of elderly patients.
{kind=link}
Patients who are “very fit” score a one on the scale, while terminally ill patients with fewer than six months to live score a nine. A patient scores higher on the scale the more dependent they are on others for basic activities based on their condition two to four weeks before admission to hospital.
Disability advocates said the scale would not take into account whether someone could achieve certain tasks with accommodations.
“That’s extremely problematic,” said Mariam Shanouda, a lawyer for the ARCH Disability Law Centre. “We are in effect saying that a prerequisite for critical care is not having a disability at all.”
Although it is just one of 13 ineligibility criteria included in the draft protocol, scoring higher on the Clinical Frailty Scale could lead to a patient being excluded from treatment in the event that the number of critical care patients exceeds a hospital’s capacity.
The protocol states that the tool would only be used to estimate chances of survival for patients with “progressive illness and generalized deterioration in health status” and not for nonprogressive conditions. But Shanouda and other advocates say the scale is inherently discriminatory against people with disabilities, no matter how it is used.
Shanouda also pointed to the fact that the scale was not designed for this purpose. Guidelines for using the Clinical Frailty Scale — published by its inventor, Dr. Kenneth Rockwood — state that it has not been validated for people under 65 years old or for people with “stable” disabilities. The government’s draft protocol anticipates using it for all adults.
On Friday afternoon, a spokesperson for the Ministry of Health said via email that the ministry is currently reviewing the latest proposal from its Bioethics Table, the government-appointed group of physicians and bioethicists enlisted to develop the triage protocol. Since the proposal is under review, the ministry is “unable” to share it publicly, she said.
The spokesperson said the ministry heard the concerns from disability rights experts regarding the Clinical Frailty Scale, but could not say whether or not it is included in the latest proposal. The new proposal includes “significant revisions, including revisions related to human rights and equity,” she said, adding that it is the result of “extensive consultation over the summer including with the Ontario Human Rights Commission as well Indigenous health leaders, disability rights experts and stakeholders representing marginalized populations and others who may be disproportionately affected by critical care triage.”
David Lepofsky, chair of the Accessibility for Ontarians with Disabilities Act Alliance, said the government’s lack of transparency is a major concern.
“This is an issue for which there should be a lot of sunshine, not secrecy,” he said. “It’s life and death.”
Lepofsky, who obtained a copy of the draft protocol during this summer’s consultations, published it on his group’s website. The province itself has not released any of the drafts or the Bioethics Table’s recommendations.
With the province now engulfed in COVID-19’s second wave and hospitals raising concerns about their capacity to handle a surge in patients, there is increasing pressure to make the triage protocol public.
On Wednesday, Ottawa MPP Joel Harden, the NDP’s critic for people with disabilities, submitted written questions in the legislature asking Health Minister Christine Elliott to make public the triage protocol.
“We needed this information months ago, but at this point it’s unacceptable that people with disabilities don’t know the answer to these questions,” Harden said in an interview. “In the event that people who are similarly affected by this virus are waiting for life-saving equipment, we certainly don’t want any assumptions made about someone’s quality of life as a person with a disability and therefore whether or not they should access a ventilator any sooner than anybody else.”
Critics of the draft protocol also say it lacks due process by not including an appeal mechanism for patients and their families.
“There is nothing in their protocol, including the revised protocol, to ensure fairness and due process,” Lepofsky said. “I’m not saying (an appeal) could go on for weeks and weeks, but we put forward in our submissions a proposal for a rapid, informal — but necessary — set of due process protections.”
Roxanne Mykitiuk, a professor at York University’s Osgoode Hall Law School and an expert in disability law and bioethics, said the triage protocol should limit its scope to assessing a patient’s ability to survive COVID-19 and not try to estimate their lifespan beyond that.
“You can’t really make that determination accurately, so let’s not try,” she said. “Let’s just make the assessment on a short-term basis.”
Mykitiuk, who was invited by the Bioethics Table to give feedback on the draft protocol and worked with the ARCH Disability Law Centre on their submissions, said the protocol should explicitly state that any triage decision must avoid discrimination and must adhere to human rights standards. “They need to expressly say that the presence of disability is not a permissible basis for giving lower priority for intensive care.”
CLINICAL FRAILTY SCALE
- Very fit — Robust, active, energetic and motivated. Regular exercise.
- Well — No active disease symptoms, but less fit than first category.
- Managing well — Medical problems are controlled, but not regularly active beyond walking.
- Vulnerable — Not dependent on others for daily help, but symptoms limit activities.
- Mildly frail — Need help in “high order” instrumental activities of daily living (IADL), such as finances, transportation and heavy housework.
- Moderately frail — Need help with all outside activities and keeping house, often need help with stairs, bathing.
- Severely frail — Completely dependent for personal care, but stable and not at high risk of dying.
- Very severely frail — Completely dependent, approaching the end of life. Typically would not recover from even a minor illness.
- Terminally ill — Approaching end of life, with a life expectancy of less than six months.
SOURCE: Geriatric Medicine Research, Dalhousie University
Brendan Kennedy is a Toronto-based social justice reporter for the Star. Follow him on Twitter: @BKennedyStar
Radio Canada October 3, 2020
(Automated translation)
Originally posted at https://twitter.com/philippedemo/status/1312757314722635776?s=21
CORONAVIRUS: THE SITUATION IN ONTARIO
Ontario’s triage protocol leaves a stir for people with disabilities
A patient stays in an intensive care unit.
The triage protocol is a guide that would allow Ontario hospitals to decide which patients would be eligible for a ventilator in the event of a shortage.
By Philippe de Montigny
Doug Ford’s government has been stealthily developing an intensive care bed management plan as Ontario prepares to face a second wave of COVID-19 that could be more fierce than the first.
The triage protocol, developed in recent months would allow Ontario hospitals to choose patients who would be eligible for a ventilator in the event of a shortage.
This protocol includes a frailty index ( clinical frailty scale in English) which is based, among other things, the life expectancy of patients, their level of independence and if they suffer from degenerative diseases.
Patients with an estimated life expectancy of less than six months would be excluded. The rest are classified according to a variety of activities they can undertake without assistance – such as eating, dressing, walking, and bathing.
It would be serious human rights violations.
David Lepofsky, Chair of the AODA Alliance
Basically, we decide who lives and who dies based on their disabilities. And we put those with the most severe disabilities at the bottom of the list says lawyer and activist David Lepofsky.
The province is already considering up to 1,000 new cases of COVID-19 every day during the first half of October, which could exacerbate the problem of hospital congestion.
A spokesperson for the Ministry of Health explained that the protocol would only be applied in the event of a sharp increase in demand for intensive care, exceeding supply and after any reasonable effort to mobilize resources in a hospital or region.
A discriminatory practice, according to experts
According to the triage protocol, the frailty index is used to predict the likelihood that a patient will die in intensive care even if a ventilator and treatment are provided.
Roxanne Mykitiuk, a law professor specializing in bioethics, maintains that a very poorly autonomous patient, who would therefore have a low score according to the index of the province, could very well survive the coronavirus.
The protocol is prima facie discriminatory against people with disabilities, she said. It has nothing to do with their state of health, nor their ability to recover from COVID.
Professor Roxanne Mykitiuk.
Roxanne Mykitiuk, professor at Osgoode Hall Law School in Toronto, believes that putting this protocol into practice would violate the Canadian Charter of Rights and Freedoms.
She points out that the fragility index was designed 15 years ago to better plan the provision of health care to people with more pressing needs. This indicator is very problematic when used to sort human lives she says.
I don’t think doctors want to make those kinds of heartbreaking choices. They want to help people survive, not decide who should die.
During consultations in March and August, Ms. Mykitiuk voiced her concerns to the province’s bioethics table, the multidisciplinary expert committee responsible for drafting the intensive care triage protocol.
She fears that the first draft of this plan may still be the watchword in the health system. The government has never clarified whether this highly problematic old draft has been revoked she said.
Doris Grinspun, director of the Registered Nurses Association of Ontario, says the Ford government had several months to plan its workforce and avoid hospital congestion, which appears to materialize this month.
This protocol is squarely determining who lives and who dies, she says. It is an unthinkable choice that is imposed on us.
The director also believes that the new measures announced on Friday do not go far enough to curb the spread of the virus. It’s too little, too late she said.
Opposition calls for debate at Queen’s Park
New Democrat accessibility critic Joel Harden is urging the Ford government to unveil its ICU triage protocol, in its current form. He submitted a written question to this effect to the Minister of Health on Wednesday.
The deputy also asked him to make public and accessible any recommendation and any report issued on this subject by the bioethics table.
We have concerns. We need answers.
In other countries, where there have been overloads, there have been absolutely shameful decisions in relation to the elderly, to people with disabilities he says.
Considering its implications, such a protocol should be passed through a bill and debated in the Legislature, said Harden.
We have fallen into a second wave of COVID. Hospitals are not overloaded at the moment, but it is quite possible, says the MP. We must now ensure that the human rights of people with disabilities are guaranteed.
The Ministry of Health says a revised version of the protocol that includes significant changes is under consideration, but refuses to release it for now.
After its consultations with experts in the rights of people with disabilities, the bioethics table recognizes that using the frailty index in the context of triage in intensive care raises important concerns replied a spokesperson for the ministry.